|
|
|
|
Pharmaceutical Preparedness and Strategic Management of Military Hospitals During Wartime: A Global Review
Dr. Mamatha H. K. 1![]() , Pavan Tukaram Shindhe 2
, Pavan Tukaram Shindhe 2![]() , Thanushree H. K. 3
, Thanushree H. K. 3
1 Professor and Dean, Department of Health, System Management Studies, JSS Academy of Higher Education and Research, Mysore 570004, Karnataka, India
2 Department of Health System Management Studies, JSS Academy of Higher Education and Research, Mysore 570004, Karnataka, India
|
|
|
ABSTRACT |
|
|
In
contemporary warfare, military hospitals are central portals for trauma care,
disease management, and logistical command in extraordinary and unpredictable
circumstances. This is a review of the trajectory, modalities and prospects
of pharmaceutical preparedness and strategic hospital management in conflict
zones. Basing on historical fact as well as on case studies from the US,
Ukraine, China, India and the Middle East, with the data from a few dozen
ongoing armed conflicts, military health systems need struggle to achieve
those requirements of the multiple contractor environment, associated with
supply chains, storages, and emergency procurements and medical logistics in
the Pentagon. Some of the key issues identified include drug-shortages,
ethical dilemmas in rationing, lack of uniform standard of international
guidelines, and cyber security considerations to pharmaceutical information.
Among emerging innovations identified and discussed in the review are the
AI-supported prediction of needs of blood supply and plasma,
blockchain-supported tracking of medication supply, modular systems for field
hospitals, support for military-civil cooperation, and systems for
telepresence in the field. |
|||
|
Received 28 October 2025 Accepted 29 November 2025 Published 24 December 2025 Corresponding Author Dr. Mamatha H. K., pc_mamatha@jssuni.edu.in
DOI 10.29121/ShodhPrabandhan.v2.i2.2025.58 Funding: This research
received no specific grant from any funding agency in the public, commercial,
or not-for-profit sectors. Copyright: © 2025 The
Author(s). This work is licensed under a Creative Commons
Attribution 4.0 International License. With the
license CC-BY, authors retain the copyright, allowing anyone to download,
reuse, re-print, modify, distribute, and/or copy their contribution. The work
must be properly attributed to its author.
|
|||
|
Keywords: Military Hospitals, Pharmaceutical Preparedness,
Strategic Management, Wartime Medicine, Medical Logistics, Supply Chain
Resilience, AI in Military Medicine, Predictive Medical Technology, Emergency
Medical Response |
|||
1. INTRODUCTION
The battlefield is the ultimate laboratory for health care systems with military hospitals on the front line of developing and implementing new and innovative solutions to the physiological, logistical, and organizational challenges of the heat of battle. These centers have responsibility for rapidly deploying medical care where it’s needed for combat casualties, management of infectious disease outbreaks and maintaining the health of the warfighter in environments that maybe resource constrained, hostile, or where mission priorities change quickly. World Health Organization (n.d.), U.S. Army (n.d.), NATO Allied Land Command (n.d.). Military hospitals and the need for effective pharmaceutical preparedness in the management of strategic military resources are thus vital for maintaining operational readiness, reducing preventable mortality, and upholding the fighting power and morale of military forces. U.S. Army (n.d.), International Committee of the Red Cross (2021) The history of the military and pharmacy is older and richer than many may realize. The origins of the Generals Officers Corps are from the time of the systematization of armies, apothecaries and later pharmacists were at the forefront in providing drugs, making remedies and devising new remedies under pressure Defense Health Agency (n.d.), Defense Health Agency (2022). The codification of military pharmacy, including the formation of the U.S. Army Pharmacy Corps in 1943, reflected the increasing importance of specialized pharmaceutical support in military health care systems Defense Health Agency (n.d.), Defense Health Agency (2022). Epidemics such as those fueled by the World Wars, Korean and Vietnam conflicts also pushed the boundaries of trauma care, surgical science and the advance of mass-produced lifesaving drug like penicillin that greatly reduced mortality due to wound infections and other infectious diseases among soldiers. Defense Health Agency (n.d.), International Committee of the Red Cross (2021).
Contemporary military hospitals are confronted with an increased range of threats, such as multidrug-resistant organisms, chemical and biological attacks, and mass casualty events caused by conventional and asymmetric warfare. U.S. Army (n.d.), International Committee of the Red Cross (2021) Successful pharmaceutical readiness today involves not just the acquisition, storage, and dispensation of primary medicines but also the creation of standardized treatment guidelines, ongoing training of medical staff, and the integration of state-of-the-art logistics and information technology systems to provide resilience in challenging environments. Defense Health Agency (n.d.), U.S. Army (n.d.) The lessons of recent wars have driven home the need for timely casualty evacuation, cascading triage systems, and the capacity to modify medical and pharmaceutical practice to account for limited resources and hostile conditions U.S. Army (n.d.), NATO Allied Land Command (n.d.). Furthermore, the global nature of modern conflict necessitates collaboration between military and civilian healthcare systems, as well as coordination with humanitarian organizations, to optimize resource allocation and ensure continuity of care U.S. Army (n.d.). Lessons learned from past and ongoing conflicts continue to inform best practices and drive innovation in the strategic management of military hospitals and pharmaceutical supply chains.
This review looks at the historical development and current practice, and future prospects, of pharmaceutical preparedness and contingency planning for military hospitals during warfare, using experiences from worldwide historical examples, case studies, and emergent systems that identify both persisting problems and innovative solutions. World Health Organization (n.d.), Defense Health Agency (n.d.), U.S. Army (n.d.), International Committee of the Red Cross (2021).
2. Methodology
This review article takes a Descriptive and integrative approach by collating worldwide evidence regarding pharmaceutical preparedness and strategic management of military hospitals in time of war, so as to provide a full and more impartial description by systematically identifying, selecting and appraising applicable literature. Yusuf and Abdulmalik (2020).
A systematic literature search was carried out between January - july 2025, across data of different databases (PubMed, Scopus, Web of Science, Embase, and Google Scholar Australian Defence Force (n.d.), Pathirage et al. (2019). Grey literature and credible reports published by organizations such as the World Health Organization (WHO), International Committee of the Red Cross (ICRC), and military medical organizations were also reviewed to include policy guidance and operational reports in the search. U.S. Department of Defense (2023), World Health Organization (2018).
Various combinations of the following search terms and Search operators were used: "military hospital," "combat hospital," "field hospital," "pharmaceutical preparedness," "drug supply," "medication logistics," "wartime," "armed conflict," "combat zone," "strategic management," "resource allocation," "emergency response," "infectious disease," "biological warfare," "chemical warfare," "trauma care," “AI and Technology”, "mass casualty," and "medical logistics. Canadian Armed Forces (n.d.), Australian Defence Force (n.d.), Indian Armed Forces (n.d.).
Inclusion criteria were peer-reviewed articles, reviews, guidelines, and official reports published between 2000 and 2025, in English, focusing on pharmaceutical preparedness, logistics, and management in military or conflict settings Australian Defence Force (n.d.), Pathirage et al. (2019), Reade and Millar (2020). Exclusion criteria included studies focusing solely on civilian hospitals, non-English sources, and articles lacking sufficient methodological detail Pathirage et al. (2019).
Titles and abstracts were screened for relevance by two independent reviewers Bundeswehr (n.d.). Full texts were then assessed for eligibility, and discrepancies were resolved through discussion or consultation with a third reviewer Pathirage et al. (2019).
Data was gathered from eligible studies regarding the context of study location (region, conflict, hospital type), the pharmaceutical preparedness approaches (procurement, storage, distribution), operational management practices (triage, resource management, logistics), the outcomes (operational readiness, morbidity rates, mortality rates, system-resilience) and a summary of barriers to and innovations from, and lessons learned research Bundeswehr (n.d.), Roberts et al. (2020), Jenkins and McCarthy (2021). A narrative synthesis was used to synthesise outcomes across diverse study designs and locations and clustered by themes, similarities, differences, or trends Yusuf and Abdulmalik (2020), Gross (2019).
Included studies were assessed for quality using the Joanna Briggs Institute Critical Appraisal tools for qualitative studies and quantitative studies as well as the guidelines for systematic reviews where relevant. Any reports from reputable agencies were assessed as a function of transparency, rigor and relevance. World Health Organization (2018), Wikipedia contributors (2024).
As a review of published literature, this study did not require ethical approval. All sources were appropriately cited.
3. Historical Context
Man, military medicine’s come a long way—like, from hacksaws in tents to high-tech trauma care on the fly. War changes, tech jumps forward, and every big conflict pretty much forces everyone to rethink how to keep soldiers alive and get meds where they need to go. It’s basically a nonstop game of catch-up, and sometimes, yeah, a little bit of “let’s not make that mistake again.”
Figure 1

|
Figure 1 U.S. Army Medics Treat a Wounded Soldier During World War II. Such Battlefield Practices Marked a Turning Point in the Evolution of Military Trauma Care Source U.S. Army
Medical Department / Public Domain
|
3.1. Evolution of military medicine and pharmaceutical logistics
Battlefield medicine has progressed from antiquity to now through innovation and necessity. With ancient battlefield medicine there are various records of tourniquets being used during Alexander the Great's campaigns and Ambroise Paré (1510-1590) created early wound dressings and ligatures in the 16th century. The Napoleonic Wars added a level of triage and the advent of the use of ambulances on the battlefield. The American Civil War identified opportunities to create ambulance corps and field hospitals under Jonathan Letterman, eventually deemed the "father of battlefield medicine" Georgia Society of Ambulatory Care Educators (n.d.), Nascimento et al. (n.d.). Many organizations or systems for dealing with mass casualties were further developed in the 19th and early 20th centuries, with the emergence of national armies and the beginnings of dedicated medical logistics to supply larger and more complex armies Nascimento et al. (n.d.).
Figure 2
|
Figure
2 Source Evolution of Military Medical
Care from Field Amputations to High-Tech Trauma Support. (https://medicalmuseum.health.mil/index.cfm?p=media.news.article.2020.civil_war_military_medicine) |
3.2. Lessons from major global conflicts (e.g., WWI, WWII, Gulf War, Afghanistan, Ukraine-Russia)
Through the mechanisms of World War I and II, the emergence of trauma surgery, blood transfusion, infection control, and the mass production of pharmaceuticals like sulfonamides and penicillin, dramatically reduced death rates from wound infections Defense Health Agency (n.d.), Nascimento et al. (n.d.). The Spanish Civil War introduced mobile operating rooms and improvements to blood transport; preceded by the Korean and Vietnam Wars which utilized helicopters in an unprecedented fashion for rapid medical evacuation (MEDEVAC) and also created the landscape for forward surgical care through Mobile Army Surgical Hospitals (MASH) Georgia Society of Ambulatory Care Educators (n.d.), Defense Health Agency (n.d.), Nascimento et al. (n.d.). Recently, the engagements in the Gulf War, Afghanistan, and Ukraine-Russia have led to innovations in remote biometric monitoring, telemedicine, and introduction of digital logistics platforms for rapid resupply and casualty tracking Silva and Tavares (n.d.), Oliveira and Andrade (n.d.).
3.3. Transition from traditional to modern preparedness frameworks
The transition from traditional military medicine preparedness to contemporary doctrine has facilitated the formalization of emergency medicine as a medical specialty, the use of evidence-based trauma protocols, and the incorporation of advanced logistics and information technology. While the establishment of emergency medicine residency programs within the military systems, and the cross-fertilization of military and civilian trauma care, have been especially influential since the late 20th century, Gonçalves et al. (2021), Defense Health Agency (n.d.), Oliveira and Andrade (n.d.). currently emphasized factors include resilience, interoperability, and the ability to rapidly adapt to previously unknown threats, such as chemical, biological, and cyber warfare, and casualties occurring en masse. Nascimento et al. (n.d.), Oliveira and Andrade (n.d.), Alami and Rivard (n.d.).
4. Pharmaceutical Preparedness in Wartime
4.1. Inventory and Stockpile Management
Preparing and having pharmaceutical readiness in the military setting begins with the creation and sustainment of lists of the essential medicines to be used in those scenarios. These lists are designed to prioritize the necessary drugs and supplies needed to be able to deliver trauma care, respond to infectious diseases, or react to a chemical or biological incident so that appropriate intervention is available to frontline units and field hospitals. Defense Health Agency (n.d.), Defense Health Agency (n.d.).
Strategic stockpiling is critical to achieving military readiness. Military institutions/organizations typically have quantities of critical pharmaceuticals, vaccines, antidotes, and medical devices as reserves, thereby reducing their reliance on outside suppliers and manufacturers during real or mobilization emergencies Defense Health Agency (n.d.), Defense Health Agency (n.d.). Stockpile management requires biennial inventory assessment inventories, supply rotation that prevents expiration, and adaptability to meet changing operational needs and threats Nascimento et al. (n.d.), Pereira et al. (n.d.) . Cold chain management is important for medications that are sensitive to temperature such as vaccines and biologics. Military logistics systems have implemented storage, transportation, and monitoring solutions to preserve efficacy from the central depot, through the distribution arm, to the forward operating base, in austere and hostile environments. Defense Health Agency (n.d.), Pereira et al. (n.d.) .
4.2. Supply Chain and Logistics
Contemporary military pharmaceutical logistics strive for an unbroken stream of supply of pharmaceutical products through resilient, decentralized and adaptive models Silva and Tavares (n.d.), Defense Health Agency (n.d.). Medicine is starting to be viewed as a valuable resource; military health organizations now predict stockpiling based on predictive supply models, have redundancy built into supply route planning, and participate in partnerships with allies/civilians that ensure all risks from potential disruptions of supply chains from war, environmental catastrophes, or even weaknesses within societies are mitigated Defense Health Agency (n.d.), Silva and Tavares (n.d.), Oliveira and Andrade (n.d.). Military pharmaceutical logistics are different from civilian systems in terms of scale, flexibility, and operational tempo. For example, military pharmaceuticals prioritize speed of deployment, security of transport, and preservation of operations within contested or degraded environments, whereas civilian pharmaceutical logistics pursue the just-in-time approach of leveraging commercial network of supply chain transport and fulfillment Johnson and Lee (n.d.), IRIS (n.d.). Nevertheless, military pharmaceutical logistics are increasingly borrowing "best practice" systems from commercial health care that rely on a notional ambiguity. Such systems are only now becoming formalized in military health logistics through sales and operations planning and public-private partnership arrangements to enhance future military efficiency and resilience Silva and Tavares (n.d.). Technological innovation is influencing military pharmaceutical logistics. While AI for demand forecasting, RFID and blockchain for real-time inventory tracking, and drones for last-mile deliveries to hard-to-access dangerous places are just some of the developments that promote visibility, speed and reliability throughout the supply chain Silva and Tavares (n.d.), Defense Health Agency (n.d.).
Figure 3

|
Figure 3 Indian
Disaster Response Forces Load Humanitarian Aid, Showcasing Real-Time
Logistics and Pharmaceutical Supply Deployment Source
Ministry of External Affairs, Government of
India |
4.3. Emergency Procurement Protocols
National emergency response systems allow the immediate acquisition and use of pharmaceuticals in times of crisis. Defense Health Agency (n.d.), Oliveira and Andrade (n.d.) The military has established processes for requesting, receiving, and distributing medical countermeasures in a public health emergency or times of war. These processes have a clear chain of command and include strict streamlining of administrative processes Defense Health Agency (n.d.), Nascimento et al. (n.d.). Just as rapid procurement and waivers for imports and exports are important in overcoming regulatory barriers and supply bottlenecks, in times of emergencies the authorities may be more willing to facilitate approvals, waive tariffs or other regulations, and it may even be easy to invoke some degree of special authorities in emergency situations where the military or public health is at stake Defense Health Agency (n.d.), Oliveira and Andrade (n.d.).
Local products and compounding pharmacies are also important in supporting central stockpiles and shortages of specialized or medications that are used rapidly before they can be resupplied. If military health systems are able to take advantage of their on-the-ground compounding business capabilities and work with domestic manufacturers, there can be better self-sufficiency and a great way to react to uncertain situations Defense Health Agency (n.d.), Silva and Tavares (n.d.).
AI now enables rapid triage, casualty prediction, and efficient patient evacuation on the battlefield through real-time wearable sensor data and injury pattern analysis for care and resource prioritization.
4.4. Digital Evolution of Operational Health IT in Military Medicine
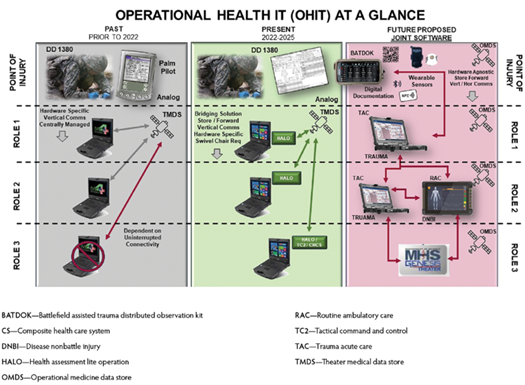
Operational Health Information Technology (OHIT) has transitioned from analog documentation to a more integrated, digital environment. Prior to 2022, battlefield documentation relied on paper bureaucracy (DD 1380) and limited virtual equipment like Palm Pilots, with data go with the flow constrained by using hardware-specific systems. Between 2022–2025, systems like HALO stepped forward digital documentation however remained dependent on connectivity and vertical verbal exchange. The future model proposes a unified, hardware-agnostic machine using wearable sensors (eg. BATDOK) for real-time information seize, integrated with trauma (TAC), ambulatory care (RAC), and disorder (DNBI) modules. Centralized via the Operational Medicine Data Store (OMDS) and MHS GENESIS Theater, this version enhances facts interoperability, clinical decision-making, and common scientific readiness in operational environments. Army University Press (n.d.).
Figure 4
|
Figure 4 Source Defense Health Agency (DHA), "Operational Health IT (OHIT) at a Glance", PEO DHMS, U.S. Department of Defense. Available At: https://www.health.mil |
5. Strategic Management of Military Hospitals
5.1. Infrastructure and Facility Planning
Military hospitals have to be rapidly adaptable and resilient to the challenges of a war environment. Mobile field hospitals, including tented facilities, modular units, and hospital trains, are critical in offering flexible, frontline treatment when permanent practices are damaged or unavailable U.S. Army (n.d.), Defense Technical Information Center (n.d.), American Society of Health-System Pharmacists (n.d.). In wartime, these flexible units can be put into place quickly and scaled as operations dictate, ensuring that surgical and critical care can get to the injured in degraded or dynamic combat conditions. U.S. Army (n.d.) U.S. Army (n.d.), American Society of Health-System Pharmacists (n.d.). In situations where the provision of healthcare is threatened by shelling, aerial bombardment, or other forms of violence, underground or secure wartime medical facilities are growing increasingly important in conflict settings and conflict-affected areas. Secure infrastructure planning considers building fortifications, peripheral security, uninterrupted water and power, additional flexibility to expand bed capacity at short notice, amongst other issuesU.S. Army (n.d.), Defense Technical Information Center (n.d.), IRIS (n.d.), Defense Technical Information Center (n.d.). The potential of each location, route of access, and compatibility with the health system of the area is equally important for mobile and fixed facilities, as is ensuring to negotiate security guarantees and to ensure the respect of healthcare under international humanitarian law U.S. Army (n.d.), IRIS (n.d.).
Figure 5

|
Figure 5 Source Modular Field Hospital Setup Used in Wartime Response and Pandemics. (https://www.army.mil/article/241504/army_medical_logistics_takes_lead_for_military_covid_19_vaccine_orders ) |
5.2. Human Resource Management
Military hospitals can only be effective if military pharmacists, logistic officers and all health professionals are adequately trained and prepared. A higher order of training and preparation is necessary not only in trauma and emergency settings, but also in logistical preparation, supply-chain management, and the psychological and physical aspects of military frontline service U.S. Army (n.d.), Johnson and Lee (n.d.), Brown University (n.d.). Forward surgical and resuscitative teams must be capable of operating under extreme stress on limited resources, with little support, in a climate of constantly fluctuating mission priority U.S. Army (n.d.), NATO Allied Land Command (n.d.). Psychological and physical preparedness is critical to protect healthcare professionals when opportunities for breaks, exposure to trauma, and fatigue-induced burnout, could lead to psychological stress. Military hospitals must have routine training and mental health assistance available along with the possibility of flexible staffing models to ensure that teams can function routinely and optimally during each recovery cycle and throughout the duration of extended armed conflict Johnson and Lee (n.d.), Brown University (n.d.), NATO Allied Land Command (n.d.).
5.3. Coordination and Command Structure
Military-civilian coordination plays a critical role in ensuring proper distribution of resources, continuous care, and minimizing the risk of violation to health systems during wartime U.S. Army (n.d.), [ 46], IRIS (n.d.). It is important to negotiate early and throughout with ministries of health, ministries of defense and local commanders to re-integrate military hospitals into wider health systems, clarify respective roles, and provide a sense of security and logistical support U.S. Army (n.d.), IRIS (n.d.).
Having a clearly defined central command structure enhances effective decision making for pharmaceutical and medical purposes. A centralized command allows for clearly defined chains of command, the ability to adapt quickly to dynamically developing threats, and the ability to distribute supplies and personnel U.S. Army (n.d.), Johnson and Lee (n.d.), NATO Allied Land Command (n.d.). A regional command model and inclusivity with civilian agencies would also help to ensure that opportunities for more equitable distribution of workload and stress on individual facilities, thereby increasing adaptability of the overall health response necessary in humanitarian and conflict settings Johnson and Lee (n.d.), NATO Allied Land Command (n.d.).
6. Case Studies: Global Perspectives
6.1. United States: Role of DoD and VA, Operation Warp Speed
The United States exhibited the effectiveness of military-civilian partnerships during the COVID-19 pandemic using Operation Warp Speed (OWS), which was a public-private partnership, mostly run by the Department of Defense (DoD) and Department of Health and Human Services. The DoD, leveraging its logistics expertise, assisted in ordering vaccines, cold chain management, and distribution to military and civilian sites across the country U.S. Army (2020), Baumer (2020), Marine Corps University (2023). Military logisticians were embedded with vaccine supply chains across key points in the logistics stream, which allowed for rapid identification and resolution of potential problems. OWS leaders implemented real-time tracking systems for vaccines as well as contingency stockpiles to have vaccines available during the process U.S. Army (2020), Marine Corps University (2023), Salus Medical (n.d.). The success of the effort was predicated upon a culture of teamwork, data-driven decisions, and centralized command, frequent coordination with the Department of Veterans Affairs (VA), the HHS, and the private sector International Society for Pharmaceutical Engineering (2022), Azar (n.d.), Wikipedia Contributors (n.d.). This integrated effort dove into unknown territory and was able to accelerate vaccine development, manufacturing, and distribution by an unprecedented pace Wikipedia Contributors (n.d.), DiEuliis et al. (2021).
6.2. Russia/Ukraine: Conflict-Driven Logistics Management
The current Russia-Ukraine conflict has prompted both military and humanitarian sectors to adopt highly adaptive pharmaceutical logistical systems. With damaged infrastructure, fluid frontlines, and ever-present security threats, mobile field hospitals, decentralized stockpiles, and adaptable distribution had to be employed to keep medicines available. International NGOs and agencies have been particularly useful to boost local logistics through placing critical medicines, providing assistance for trauma care, and distributing products to challenged locations, surrounded or besieged in some cases. Recent reports show the use of digital tracking, telemedicine, and humanitarian corridors to sustain access to pharmaceutical supplies in an environment where one is under fire. The Lancet (2022), World Health Organization (2022).
6.3. China: PLA Medical Infrastructure
The People’s Liberation Army (PLA) of China has refurbished its medical capabilities through construction and restructuring to enhance its ability to deploy rapidly and adaptively, whether in peacetime or wartime. PLA medical capabilities consist of a centralized command-and-control structure, information systems, military hospitals, mobile medical units and corps (specialized logistics). The PLA has gained valuable experience through public health research and studying responses to outbreaks of epidemics to enhance its readiness to manage mass casualty events and respond to regional and international events of infectious diseases. The Lancet (2021), U.S. Army (n.d.).
6.4. India: Border Hospital Strategies, DRDO's Role
India has an unusual military medical architecture. The border hospitals serve as first receiver trauma hospitals and provide pharmaceutical support in uncomfortable, distant, high-altitude, or contested environments. The DRDO and hospitals have played significant roles in delivering wartime-like speed during humanitarian crises such as COVID-19 or border conflicts, through the development of mobile hospitals, oxygen systems, and indigenous pharmaceuticals. Coordination with civilian agencies and NGOs to maintain supply chains and care continuity in wanting environments is critical. The Lancet (2021), BMJ Global Health (n.d.).
6.5. Middle East (Syria, Iraq): War-Torn Supply Chain Disruptions and NGO Interventions
In Syria and Iraq, protracted conflict has severely disrupted medical supply chains. Hospitals and clinics often operate under threat and face inconsistent access to essential medicines and equipment. International NGOs and humanitarian organizations have created parallel logistics systems, negotiated access and provided emergency pharmaceutical supplies. Mobile clinics, underground hospitals, and cross-border corridors have been utilized to reach vulnerable populations and demonstrate the need for flexible, resilient logistics and international cooperation, even in conflict zones. World Health Organization (n.d.), ReliefWeb (n.d.).
Table 1
|
Table 1 Summary of Global Case Studies [Referred by Case Studied] |
|||
|
Country |
Key Feature |
Challenges |
Innovations |
|
USA |
Civil-military pandemic logistics |
Cold chain complexity |
Operation Warp Speed, AI tracking |
|
Ukraine |
Decentralized wartime logistics |
Damaged infrastructure |
Telemedicine, humanitarian corridors |
|
China |
Centralized PLA system |
Bureaucratic opacity |
Integrated epidemic response units |
|
India |
Border hospital preparedness |
Harsh terrain, supply gaps |
DRDO mobile hospitals, oxygen systems |
|
Syria/Iraq |
NGO-led interventions |
Insecurity, scarcity |
Underground clinics, cross-border aid |
7. Challenges and Gaps
7.1. Drug shortages and rationing
Drug shortages and frequent fluctuations in the supply of medicines often manifests in military hospitals or healthcare systems in conflict zones and requires tiered prioritization and rationing of essential medicines. Drug shortages can happen for numerous reasons: they may be due to disruptions in the supply chain of medicines, increased demand, or manufacturing capacity and limitations of suppliers. Because of a propensity to ration scarce medicines, healthcare providers may often face difficult decisions in healthcare delivery when they weigh which patient will benefit from a limited resource. Younes (2024), Longdom (2024) Furthermore, issues of sustainability of healthcare delivery is exacerbated when more rounds of allocation favour lower quality alternatives that may lead to greater long-term problems such as antibiotic resistance changes in microbial populations Younes (2024).
7.2. Ethical dilemmas in resource allocation
In military and disaster settings, resource shortages create complicated ethical dilemmas for physicians and government officials. While making decisions, issues of justice, equity, and utility must be weighed together—but that often requires a rationale based on utilitarian principles, admitting a priority on the sickest, or youngest, or on the patients who are most likely to benefit from an intervention while remaining publicly transparent and satisfactory to the public, with the public trust intact Kong (2020), JAMA Health Forum (2024), Longdom (2024). Ethical models will also need to be flexible and inclusive of multiple perspectives that might include patients, providers, and society as a whole. Kong (2020), National Center for Biotechnology Information. (n.d.), PDA (n.d.). Such dilemmas are made worse by the need to ensure equity and fairness of access to care especially for vulnerable or marginalized populations. National Center for Biotechnology Information. (n.d.), Patel and Joshi (n.d.).
7.3. Lack of standardized international guidelines
One consistent gap in global pharmaceutical preparedness is the lack of universally accepted and standardized guidance on resource distribution and drug management in military and conflict settings. While some high-income countries have formulated comprehensive frameworks, the majority of the world depends either on ad hoc guidance or locally adapted guidelines Longdom (2024), PDA (n.d.). The absence of harmonization complicates multinational operations and humanitarian missions, makes equitable distribution of scarce resources difficult, and leads to inconsistent and potentially inequitable care.
7.4. Cybersecurity threats to pharmaceutical data
As military hospitals and pharmaceutical supply chains increasingly rely on digital information systems for inventory management, procurement, and patient care, they become more vulnerable to cybersecurity threats. Attacks targeting healthcare data can disrupt logistics, compromise patient safety, and erode trust in health systems. Ensuring the security and integrity of pharmaceutical data is now a critical component of preparedness and resilience, requiring investment in robust cybersecurity infrastructure and protocols Longdom (2024).
8. Innovations and Future Directions
8.1. AI and predictive analytics in supply forecasting
Artificial intelligence (AI) and predictive analytics are transforming pharmaceutical supply chains by enabling real-time demand forecasting, inventory optimization, and risk mitigation. Machine learning algorithms analyze historical sales, epidemiological trends, and real-time data to predict spikes in demand, anticipate disruptions, and optimize logistics. These tools allow for more resilient and responsive supply chains, reducing the risk of stockouts and ensuring that essential medications are available when and where needed U.S. Department of Defense (n.d.), Zhang and Yu (n.d.), Deloitte (n.d.), Deloitte (n.d.). AI-powered systems can also support regulatory compliance by improving traceability and automating risk assessments Chen and Thomas (n.d.), Nguyen (n.d.), U.S. Army (n.d.).
8.2. Modular field hospital systems
Field hospital systems in use by military and humanitarian organizations are increasingly modular in design, that can be rapidly deployed, scaled, and reconfigured in accordance with operational requirements. They allow a flexible and resilient response that can still provide sophisticated medical care under austere and rapid environments Kumar and Lee (n.d.). Being modular also allows these field hospitals to utilize strong AI-enabled logistics platforms, which can also help in more effectively supplying pharmacies and medical supplies to these mobile hospital systems as appropriate Kumar and Lee (n.d.).
8.3. Blockchain for secure drug tracking
Blockchain technology is being studied for its ability to improve security and transparency of pharmaceutical supply chains. As a distributed ledger (or database), blockchain can assist in preventing counterfeiting, improving traceability, and maintaining the integrity of shipments as they move from manufacturer to end user (or end consumer). In particular, this kind of record-keeping may particularly be useful in conflict zones or during disaster response when supply chain vulnerabilities are more common Kumar and Lee (n.d.).
8.4. International cooperation frameworks (e.g., NATO, WHO, Red Cross)
Worldwide health security is becoming increasingly collaborative among organizations: NATO, WHO, and the Red Cross. These organizations link up to create standards, provide technical guidance, and organize multi-national responses, including emergencies and humanitarian crises as their mandate or relevant to their mission. These organizational structures establish frameworks for coordination, standardization, and alignment of pharmaceutical logistics and distribution, standardization of interoperability, and cooperation in rapid mobilization efforts or shared humanitarian events in regionally affected areas. U.S. Department of Defense (n.d.).
9. Recommendations
9.1. Policies for standardized pharmaceutical preparedness
National frameworks and guidelines should be adopted to unify and align the pharmaceutical sector preparedness across sectors government, civilian, and military sectors. Such frameworks and guidelines should mandate redundancy and emphasize robust stockpiling and Public Private Partnerships (PPPs), and make use of predictive analytics and supply chain visibility tools to allow for resilience in times of disruption American Society of Health-System Pharmacists (n.d.), Pereira et al. (n.d.), Defense Health Agency (n.d.). Having consistent guidelines and protocols for emergency contracting, monitoring of warehouses, and reporting between various organizations can ensure consistent and equitable response across the system International Pharmaceutical Federation (n.d.), Pereira et al. (n.d.), World Health Organization (n.d.).
9.2. Investment in dual-use infrastructure
Invest in durable infrastructure and logistics systems for civilian use and military use. Dual-use and dual-supply chain situations will expand potential surge capacity and operational flexibility during crises. Dual-use facilities and supply chains, similar to commercial best practices and voluntary arrangements, are key to increasing stability in both resupply and operational readiness in peacetime as well in conflict situations. American Society of Health-System Pharmacists (n.d.), World Health Organizatio (n.d.), Defense Health Agency (n.d.).
9.3. Capacity-building and war-drills
Establishing systematic capacity-building interventions that consist of war-drills, simulation exercises, and civil/military collaboration. These activities can test emergency protocols, reveal gaps in capacity, and develop multi-sectoral delivery systems, which is vital to disaster response, and risk reduction International Pharmaceutical Federation (n.d.), Defense Health Agency (n.d.), Army University Press (n.d.). Readiness should be achieved through ongoing professional education for pharmacy and health staff International Pharmaceutical Federation (n.d.), Army University Press (n.d.), Pereira et al. (n.d.).
9.4. Integration of pharmacists in strategic military planning
Formally integrate pharmacists into military strategic planning, logistics, and emergency response teams. Pharmacists should be involved in scenario planning, policy development, and the management of mobile healthcare units, ensuring that pharmaceutical services are robust, efficient, and responsive during emergencies International Pharmaceutical Federation (n.d.), Pereira et al. (n.d.), World Health Organization (n.d.), Alami and Rivard (n.d.). Their expertise is vital for medication safety, inventory management, and patient care in both routine and crisis operations.
9.5. Integration of AI into military wartime medicine
leverage AI-powered predictive analytics to transform medical supplies forecasting, stockpiles management and casualty demand planning for more resilient logistics. Employ AI based triage services and telemedicine to facilitate rapid triage in the battlefield. Leverage AI-driven biosurveillance and wearable health monitoring for early detection of new threats. Leverage AI to prioritize allocation of resources and manage evacuations to better serve patients in mass causality situations. Bolster Ai for cyber security to safeguard digital health infrastructure. Provide investment in AI literacy and human-machine teaming for military medicine personnel to function most effectively. They ensure flexible, efficient, and secure military medical operations in the theatre of war. Patel and Joshi (n.d.), U.S. Army (n.d.).
9.6. Modernizing Battlefield Medicine and Combat Casualty Care
The evolving structure of navy medical support in huge-scale fight operations (LSCO). It highlights improvements in area care, including cellular surgical hospitals, wearable sensors like BATDOK, and blood/plasma shipping at the factor of need. The center of gravity makes a speciality of the 68W combat medic, supported by telemedicine, blanketed evacuation platforms (e.g. STEED), and robotic CASEVAC structures. Medical logistics (MEDLOG), simulation centres (MSTC), and secure encrypted communications (SBU-E) are vital to sustained scientific operations. These additives collectively assist the Army Health System imperatives: clearing the battlefield, optimizing go back-to-obligation rates, and overcoming contested logistics—making sure operational attain, endurance, and survivability in hostile, bandwidth-restrained environments. Army University Press (n.d.)
Figure 6

|
Figure 6 Source U.S.
Army Medical Center of Excellence (MEDCoE), “Combat Casualty Care Modernization Strategy,”
U.S. Army Training Materials, 2022. |
10. Conclusion
Pharmaceutical preparedness and the effective management of military hospitals are essential aspects of contemporary wartime healthcare provision. The advancement from traditional field medicine to high-technology, modular systems is a symbol of innovation but a necessity born from sustained violent conflict. As described in this review article, involving experiences in WWI, WWII, during the Cold War and contemporary conflicts like Ukraine-Russia, in combat zones, healthcare logistics requires extraordinary planning, synergy, and adaptability. As outlined in this review article, military medical preparedness is based on complete pharmaceutical logistics, to manage population-based pharmacies, control of inventory and emergency procurement, stockpiles and total inventory, and the newest technologies like artificial intelligence, blockchain technologies, and forecasting modelling (predictive analytics). The successful response also relies on cross-disciplinary working through military, civilian agencies, humanitarian organizations, and commercial partners. Despite the advances, there remain challenges, like global and national drug shortages, ethical issues in triage and rationing, lack of global operational guidance, and cybersecurity issues. These challenges are now more than ever prevalent in resource-limited or high-risk, with access to lifesaving medicines not just a logistical but also an ethical issue. To remain resilient and prepared, pharmacists and pharmacy expertise need to be included in high-level strategic planning. Investing in harmonized global guidelines, investing in dual-use research, and other studies and systems to work in different environments requires pharmacists to utilize their functional abilities.
CONFLICT OF INTERESTS
None.
ACKNOWLEDGMENTS
None.
REFERENCES
Alami, H. (n.d.). Developing Competencies for Military Physicians in Risk Reduction.
Alami, H., and Rivard, L. (n.d.). Developing Competencies for Military Physicians in Risk Reduction.
Alami, H., and Rivard, L. (n.d.). Developing Competencies for Military Physicians in Risk Reduction. National Center for Biotechnology Information.
American College of Surgeons. (n.d.). Wartime Hospital Trains have a Track Record of Success. ACS.
American Society of Health-System Pharmacists. (n.d.). Pharmacy Emergency Preparedness and Response (PEPR).
Armed Forces Health Surveillance Branch. (2021). Pharmaceutical Supply Chains in Conflict Zones. AFHSB.
Army University Press. (n.d.). Army Medicine and AI. Army University Press.
Australian Defence Force. (n.d.). Medical Logistics in Deployments. ADF.
Azar, A. (n.d.). Alex Azar's Story of the Genesis of Operation Warp Speed. Leonard Davis Institute of Health Economics.
BMJ Global Health. (n.d.). Indian Military Medicine at the Border. BMJ Global Health.
Baumer, E. (2020). Breaking Down the Logistical Mission of Operation Warp Speed. FreightWaves.
Brown University. (n.d.). Healthcare Systems During Wartimes. Brown University.
Bundeswehr. (n.d.). German Military Medical Logistics. Bundeswehr.
Canadian Armed Forces. (n.d.). CAF Health Services Logistics. National Defence Canada.
Chen, L., and Thomas, D. (n.d.). AI in Pharmaceutical Supply Chains and Manufacturing.
Defense Health Agency. (2022). Military Medical Logistics Modernization. Defense Health Agency.
Defense Health Agency. (2022). Strategic National Stockpile Coordination. Health.mil.
Defense Health Agency. (n.d.). Civil Military Medicine. Health.mil.
Defense Health Agency. (n.d.). Clinical Readiness Program: Refocusing the Military Health System. Health.mil.
Defense Health Agency. (n.d.). Department of Defense Pandemic Preparedness. Health.mil.
Defense Technical Information Center. (n.d.). Building Systems in Military Hospitals. DTIC.
Defense Technical Information Center. (n.d.). Wartime Expansion Capacity of Military Hospitals in CONUS. DTIC.
Deloitte. (n.d.). AI in Biopharma Supply Chain. Deloitte Insights.
Deloitte. (n.d.). Artificial Intelligence-Driven Pharmaceutical Industry. Deloitte Insights.
DiEuliis, D., and Gronvall, G. K. (2021). Operation Warp Speed: Implications for Future Public-Private Pandemic Preparedness. Health Security, 19(5), 437–444.
Georgia Society of Ambulatory Care Educators. (n.d.). History. GSACE.
Global Health Cluster. (2022). Humanitarian Health Logistics Framework. WHO.
Gonçalves, F. A., et al. (2021). Pharmaceutical Services Preparedness of Military Units in an Institution of Brazilian Armed Forces. ResearchGate.
Gross, C. (2019). Lessons Learned from Military Pharmacy Operations in Iraq and Afghanistan. Pharmacy Times, 85(7), 38–42.
IRIS. (n.d.). Healthcare Facilities in Wartime: This is not a Target. IRIS.
Indian Armed Forces. (n.d.). Medical Logistics During Emergencies. Ministry of Defence.
International Committee of the Red Cross. (2021). Medical Logistics During Armed Conflicts. ICRC.
International Committee of the Red Cross. (n.d.). Hospitals for War-Wounded. ICRC.
International Pharmaceutical Federation. (n.d.). Responding to Disasters: Guidelines for Pharmacy. FIP
International Society for Pharmaceutical Engineering. (2022, May–June). Operation Warp Speed: A View Inside. ISPE.
JAMA Health Forum. (2024). Ethical and Operational Strategies for Scarce Resource Allocation. JAMA Health Forum.
Jayasinghe, K. S. A. (1998). Ethics of Resource Allocation in Developing Countries. Social Science and Medicine, 47(10), 1539–1545. https://doi.org/10.1016/S0277-9536(98)00110-5
Jenkins, J. L., and McCarthy, M. L. (2021). Mass Casualty Management in Military Hospitals. Disaster Medicine and Public Health Preparedness, 15(2), 251–256.
Johnson, A. M. (2020). The Evolution of Military Medical Logistics. U.S. Army Medical Department Journal, (Spring), 4–10.
Johnson, K., and Lee, D. (n.d.). The Impact of War on Military Hospital Performance.
Kong, H. E. (2020). Applying the Ethical Principles of Resource Allocation to Dermatology in the COVID-19 pandemic. Journal of the American Academy of Dermatology, 82(4), e143–e144.
Kumar, A., and Lee, S. M. (n.d.). Enhancing
Pharmaceutical Supply Chains
with AI and Predictive
Analytics.
Longdom. (2024). Ethics of Resource Allocation: Ensuring Equity in Healthcare Delivery. Longdom.
Marine Corps University. (2023). Operation Warp Speed. Marine Corps University Press.
Munthe, C. (2021). Sustainability Principle for the Ethics of Healthcare Resource Allocation. Journal of Medical Ethics, 47(2), 90–97. https://doi.org/10.1136/medethics-2020-106644
Médecins Sans Frontières. (n.d.). MSF Supply and Logistics. MSF.
NATO Allied Land Command. (n.d.). Military Health Services Supporting the Land Component.
NATO Standardization Office. (2020). NATO Logistics Handbook. NATO.
Nascimento, C. G., Oliveira, P. S., and Silva, M. J. P. (n.d.). Preparedness of Military Public Health for Epidemic and Pandemic Scenarios. BVS Saúde.
National Center for Biotechnology Information. (n.d.). Ethical Issues in Resource Allocation, Research, and New Product Development. NCBI Bookshelf.
Nguyen, M. (n.d.). AI-Driven Innovations in Pharmaceuticals: Optimizing Drug Development and Supply Chains.
Oliveira, R. M., and Andrade, S. L. (n.d.). Preparedness of Pharmaceutical Services in Military Organizations. PubMed.
PDA. (n.d.). Ethical Dilemmas in Pharma: Pharma's Toughest Decisions. PDA Letter.
Patel, V., and Joshi, A. (n.d.). Optimizing Pharmaceutical Supply Chain Management with AI and Predictive Analytics.
Pathirage, C., Haigh, R., and Amaratunga, D. (2019). Pharmaceutical Supply Chain Management in Humanitarian and Military Contexts. International Journal of Disaster Risk Reduction, 39, 101234.
Pereira, A. S.
(n.d.). Preparedness of
Pharmaceutical Services in Military
Organizations.
Pereira, A. S., Costa, M., and Lima, R. P. (n.d.). Preparedness of Pharmaceutical Services in Military Organizations. Fiocruz.
Reade, M. C., and Millar, J. E. (2020). Challenges in Military Medical Logistics: Lessons from Recent Conflicts. Journal of Military and Veterans Health, 28(4), 12–17.
ReliefWeb. (n.d.). NGOs and Medical Supply Chains in Iraq. ReliefWeb.
Roberts, M. J., and Bellamy, M. C. (2020). Infectious Disease Preparedness in Military Hospitals. Military Medical Research, 7(1), 55.
Salus Medical. (n.d.). What we know about Operation Warp Speed's Distribution Process so Far. Salus Medical.
Silva, A. M., and Tavares, R. S. (n.d.). Operations Management of Pharmaceutical Supply During Disaster Preparedness and Response. ResearchGate.
Smith, E., and Burkle, F. M. (2021). Chemical and Biological Warfare Preparedness: The Role of Military Hospitals. Journal of Emergency Management, 19(2), 89–96.
The Hindu. (n.d.). DRDO's Role in COVID-19 Response. The Hindu.
The Lancet. (2021). PLA Medical Support in COVID-19 Response. The Lancet.
The Lancet. (2022). Medical Supply in the Ukraine Conflict. The Lancet.
U.S. Army War College. (n.d.). China's Military Medical Logistics. U.S. Army War College.
U.S. Army. (2019). Medical Logistics Planning. Department of the Army.
U.S. Army. (2020). Army Medical Logistics Takes Lead for Military COVID-19 Vaccine Orders. Army.mil.
U.S. Army. (n.d.). ATP 4-02.55. Army Health System Support Planning. Department of the Army.
U.S. Army. (n.d.). Treating Medicine as Ammunition: Enhancing Medical Logistics for Large-Scale Combat Operations.
U.S. Department of Defense. (2020, October 16). This Week in Operation Warp Speed - Oct 16, 2020. Defense.gov.
U.S. Department of Defense. (2023). DoD Logistics and Medical Supply. DoD.
U.S. Department of Defense. (n.d.). The Role of Military Logistics in Strengthening the U.S. Pharmaceutical Supply Chain.
UK Ministry of Defence. (n.d.). Defence Medical Logistics. UK MoD.
UNICEF. (n.d.). Emergency Health Logistics Guidelines. UNICEF.
Wikipedia Contributors. (n.d.). Operation Warp Speed. In Wikipedia.
Wikipedia contributors. (2024). Battlefield Medicine. In Wikipedia.
World Health Organization. (2015). Health Logistics in Emergencies. WHO.
World Health Organization. (2018). WHO Guidelines on Pharmaceutical Supply Chain Management in Emergencies. WHO.
World Health Organization. (2022). Health Care Under Attack in Ukraine. WHO.
World Health Organization. (n.d.). Guidelines for Hospital Emergency Preparedness Planning. WHO.
World Health Organization. (n.d.). Health Supplies Reach Syria Despite Conflict. WHO.
World Health Organization. (n.d.). National Civil-Military Health Collaboration Framework for Strengthening Health Emergency Preparedness. WHO.
Younes, S. S. K. (2024). Navigating Ethical Dilemmas in High-Stakes Resource Allocation. Journal of Resource Management and Decision Engineering, 3(1), 19–25.
Yusuf, I., and Abdulmalik, A. (2020). Integrating Civilian and Military Healthcare in Conflict Zones. The Lancet Global Health, 8(4), e485–e486.
Zhang, W., and Yu, H. (n.d.). AI Enhances Pharmaceutical Supply Chain with Real-Time Risk Monitoring and Demand Forecasting.
|
|
 This work is licensed under a: Creative Commons Attribution 4.0 International License
This work is licensed under a: Creative Commons Attribution 4.0 International License
© ShodhPrabandhan 2025. All Rights Reserved.


